On September 11, 2021, Yan Yang, Director of Department of Cardiovascular Surgery of the First Affiliated Hospital of Xi 'an Jiaotong University (XJTU) led the team to officially launch the clinical trial of "balloon-expandable interventional valve-in-valve implantation", which is the first interventional valve applied in clinical trial stage around the globe. Interventional minimally invasive valve-in-valve implantation was successfully performed for 5 patients via different approaches (femoral artery, apex, right subaxillary incision+right atrium and internal jugular vein) using three valves (aortic valve, mitral valve and tricuspid valve), setting a new record for single-center interventional valve-in-valve implantation in China on a single day. Department of Cardiovascular Surgery in our hospital is the only affiliation participating in this research project in Northwest China. The success of these 5 cases repeatedly signifies the potent strength of our hospital in the field of interventional valve implantation.

To guarantee the success of surgery, Director Yan Yang and Professor Li Yongxin led the team to carefully and fully deliver preoperative and postoperative evaluation, explicitly design the surgical approaches and regimens through the imaging data, such as cardiac CTA and echocardiography, and work out comprehensive emergency plans. Four different implantation approaches were designed for 5 patients, including 1 case of internal jugular vein, 1 femoral artery, 2 cardiac apex and 1 right subaxillary incision+right atrium, respectively.
Case 1 Tricuspid valve-in-valve implantation via internal jugular vein
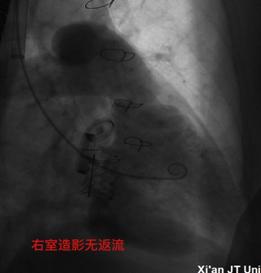
The patient, aged 69, had undergone tricuspid bioprosthetic valve replacement and implanted with a HANCOCK II 29# valve. The STS score was 11.75%, who was graded as a high-risk patient for surgical valve replacement. Preoperative cardiac ultrasound showed that the original tricuspid valve was decayed, the leaflets were prolapsed, and the tricuspid valve was slightly narrowed with moderate regurgitation. According to detailed evaluation before operation, the coaxiality of femoral vein approach was not ideal. Hence, the right internal jugular vein approach was chosen to implant the 27# Renato balloon-expandable valve-in-valve during the operation. After the successful release, the valve normally functioned, and no obvious regurgitation was observed within or surrounding the valve. The average pressure difference across the valve was 2.8mmHg. This is also the third case of this surgical approach in China.

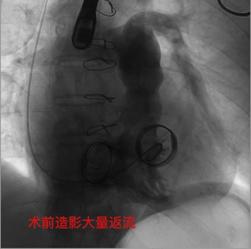
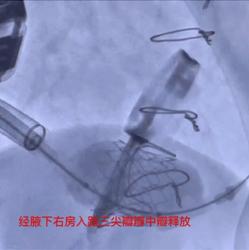
Case 2 Tricuspid valve-in-valve implantation via the right atrium
The patient, aged 68, had received tricuspid valve replacement with a BalMedic 29# valve combined with mechanical mitral valve replacement. The STS score was 9.69%, who was regarded as a high-risk patient for surgical valve replacement. Preoperative cardiac ultrasound indicated a large quantity of regurgitation of the original tricuspid bioprosthetic valve. According to explicit preoperative evaluation, the coaxiality of the femoral vein approach was not ideal, and the right internal jugular vein was seen with scarring stenosis because the patient had undergone two surgeries via this approach. Consequently, the right subaxillary small incisional approach was selected intraoperatively, and a 27# Renato balloon-expandable valve was implanted through the right atrium puncture. After the successful release, the valve function was normal, and no evident regurgitation was noted within and surrounding the valve. The average pressure difference across the valve was 0.5mmHg. This is also the second case of such surgical approach in China.
Case 3 Valve-in-valve implantation via transapical mitral valve
The 78-year-old patient had undergone mitral valve replacement and implanted with a HANCOCK II 27# valve. The STS score was 26.93%, who was classified as a high-risk patient for surgical valve replacement. Preoperative cardiac ultrasound showed that the biological valve of the original mitral valve was destroyed, the valve leaflets were obviously thickened and deformed with extremely poor valve closure and a large quantity of regurgitation could be observed. According to comprehensive evaluation before operation, 25# Renato balloon-expandable valve-in-valve implantation was performed via the cardiac apical approach. No obvious regurgitation was noted within and surrounding the valve, and the average pressure difference across the valve was 2.6mmHg.
Case 4 Mitral valve-in-valve implantation via cardiac apex
The patient, aged 60, had undergone mitral valve replacement and implanted with a HANCOCK II 25# valve. The STS score was 8.18%, who was graded as a high-risk patient for surgical valve replacement. Preoperative cardiac ultrasound showed that the original mitral valve was decayed, the valve leaflets were obviously prolapsed, the valve closure was extremely poor, and a large amount of regurgitation was seen. According to full evaluation before operation, 23# Renato balloon-expandable valve was implanted through the apical approach, and the valve function was normal after successful release, with no obvious regurgitation within and around the valve. The average pressure difference across the valve was 2.6mmHg.
Case 5 Aortic valve-in-valve implantation via femoral artery
The patient, aged 71, suffered from chest pain and shortness of breath for half a year, which were worsened for 1 month. The patient had undergone aortic valve bioprosthetic valve replacement and implanted with a HANCOCK II 21# valve. Preoperative cardiac ultrasound revealed that the biological valve of the aortic valve was decayed, the aortic valve was severely narrowed with moderate insufficiency with a peak velocity of 3.8m/s. The mean pressure difference across the valve was 23mmHg. The STS score was 8.046%, who was a high-risk patient for surgical valve replacement. Intraoperative implantation of 19#Renato balloon-expandable valve was performed via the femoral artery. After successful release, the valve function was normal and the coronary artery opening was unobstructed. The peak velocity was decreased to 2.5m/s and the average pressure difference across the valve declined to 12mmHg.
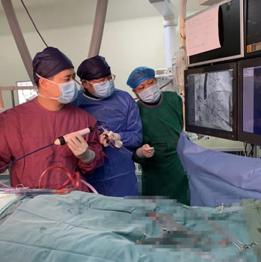
With intimate cooperation of Department of Anesthesiology and Perioperative Medicine, Interventional Operating Room and Echocardiography Room, 5 operations were successfully completed for 10 h. According to the established plans, the implantation surgeries were successfully conducted via different surgical approaches, with accurate X-ray positioning, precise catheterization and accurate valve release. All 5 patients were removed from the ventilators within postoperative 6 h, and transferred to general ward for further rehabilitation treatment the next day. Echocardiography showed that the new valve functioned normally. No regurgitation was observed within and surrounding the valves. The cardiac function of these patients was significantly improved.