Recently, Department of Anesthesiology and Perioperative Medicine of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU) has continually optimized the anesthesia management of rigid bronchoscope-assisted diagnosis and treatment by adjusting the staff allocation, updating the equipment and site, making full preoperative preparations, familiarizing with surgical procedures, strengthening intraoperative monitoring, closely observing postoperative recovery and complications. The department closely cooperated with Department of Respiratory Medicine to apply the innovative anesthesia technique characterized with “low hypoxemia, low CO2accumulation, low intraoperative cough and rapid awakening” to realize routine use of bronchoscope-assisted diagnosis and treatment in outpatients, constantly strengthen the level of comfort during diagnosis and treatment and improve the degree of satisfaction of patients with medical experience.
Rigid bronchoscope-assisted diagnosis and treatment is an important grade IV interventional procedure in outpatients. However, rigid bronchoscope-assisted diagnosis and treatment has not been routinely implemented in outpatients of our hospital due to technical bottlenecks, such as low blood oxygen, CO2accumulation and slow intraoperative awakening, management factors including understaff and lack of special recovery room as well as equipment constraints. Only 3 cases have been carried out in our hospital.
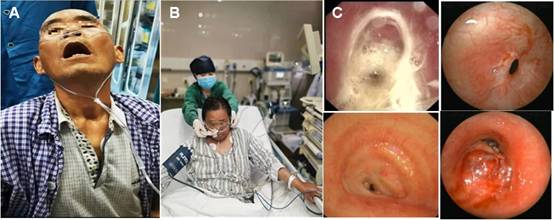
Patients with airway obstruction showed orthopnea, and severe stenosis of central airway could be seen under endoscope.
Patients with complex central airway stenosis constantly present with orthopnea complicated with vital organ dysfunction. If not treated in time, it will cause suffocation and death at any time, which seriously threatens the lives of patients. To meet the urgent rehabilitation needs of patients with airway stenosis and development needs of interventional pneumology, Department of Anesthesiology and Perioperative Medicine started to deploy and promote the implementation of outpatient bronchoscope-assisted anesthesia in our hospital at the beginning of 2021, provided comprehensive equipment and material support, and appointed Gao Wei, Deputy Chief Physician to be responsible for comfort diagnosis and treatment in outpatients.

Department of Anesthesiology and Perioperative Medicine is delivering work arrangement for bronchoscope-assisted diagnosis and treatment during meeting
With tremendous support of Wang Qiang, Director of Department of Anesthesiology and Perioperative Medicine and Li Manxiang, Director of Department of Respiratory Medicine, Deputy Chief Physician Gao Wei launched the implementation of rigid bronchoscope-assisted diagnosis and treatment in outpatients in April, 2021. She fully analyzed and learned the experience from other hospitals at home and abroad, optimized the diagnosis and treatment conditions of existing outpatient endoscopy room and constantly delivered exploratory practice with the members of diagnosis and treatment team. To resolve the issues of effect of intraoperative choking upon endoscopic operation and slow postoperative awakening, diagnosis and treatment team formulated an anesthesia administration regime of "high analgesia, moderate sedation, personalized muscle relaxation, auxiliary local anesthesia in airway and comprehensive antagonism", which realized the closed-loop accurate anesthesia effect of "no intraoperative choking and awakening immediately after withdrawal of endoscope" in bronchoscope-assisted diagnosis and treatment, and significantly improved clinical safety and efficiency of bronchoscope room in outpatients. Patients were diagnosed the obstruction of central airway complicated with poor lung function reserve. In addition, rigid bronchoscope not only occupies the airway, but also requires the inhaled oxygen concentration to be lower than 40% to prevent the incidence of airway fire during thermal treatment, which leads to ventilation problems, such as hypoxemia and CO2accumulation. The diagnosis and treatment team formulated a ventilation support regime of "nasal oxygen supply at a high flow rate before placement of rigid bronchoscope, breathing closed-loop after placement of rigid bronchoscope, anesthesia machine controlling normal breathing frequency, and individualized real-time adjustment of breathing parameters and patterns”, thereby lowering the incidence of intraoperative hypoxemia and CO2accumulation.

Li Manxiang, Director of Department of Respiratory Medicine, and Gao Wei, Deputy Chief Physician from Department of Anesthesiology
and Perioperative Medicine,performed rigid bronchoscope-assisted diagnosis and treatment for patients
This innovative anesthesia technique characterized with "low hypoxemia, low CO2accumulation, low intraoperative cough and rapid awakening" has been formulated through countless clinical exploration and improvement, which decreased the incidence of hypoxemia, CO2accumulation and intraoperative cough, and even the incidence of intraoperative hypoxemia was significantly lower than that before operation. The highest CO2partial pressure during operation did not significantly differ from preoperative level, which was also lower than the lowest CO2partial pressure during routine anesthesia as described in previous literature. After withdrawing the rigid bronchoscope and replacing the laryngeal mask to assist ventilation, it only took approximately 7 min to reach the requirement of extubation and roughly 25 min to fully awake and leave the recovery room.
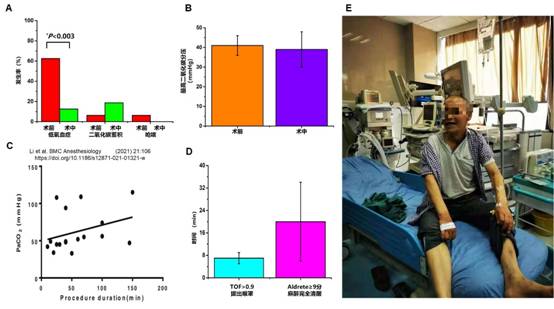
The patient is talking with medical staff at ease after the ventilation is significantly improved
With the support from Department of Anesthesiology and Perioperative Medicine, Department of Respiratory Medicine has completed the technical training for all attending physicians or titles above. Rigid bronchoscope-assisted diagnosis and treatment has been part of routine work in outpatients, 3 days every week. In addition to routine bronchoscopic examination, more than 20 cases of rigid bronchoscope-assisted diagnosis and treatment can be completed on a monthly basis.